With the powers of the executive of the Medical Council of India (MCI) being handed over to a select panel of eminent doctors, there is a new expectation that we will see dramatic improvements in medical education. Certain facts, however, need to be kept in mind before one becomes overly optimistic.
The MCI - a body of medical practitioners made up of elected representatives as well as nominees of the government (both central & state) and universities offering medical education - makes regulations governing medical education, but only with the concurrence of the Central Government. In theory, MCI is autonomous, and represents the interests of the medical profession. In practice, the MCI executive, corrupt or otherwise, has all along only implemented government policy. Examining recent regulation changes will bear this out.
Corporate medical schools
In February 2010 the MCI announced a major change in the regulation governing the establishment of medical colleges. With this change, corporate entities were permitted to open medical colleges. The new regulation also carried the following warning: "permission shall be withdrawn if the colleges resort to commercialization". Since the regulation does not elaborate on what constitutes "resorting to commercialization", this will presumably be a matter left to the discretion of the Government.
A basic requirement for a new medical college is a pre-existing hospital that will serve as a teaching hospital. Corporate entities have hospitals in the major metros and that is where they will have to locate medical colleges. The earlier mandated land requirement for a medical college campus, a minimum of 25 acres of contiguous land, cannot be fulfilled in the metros. Not surprisingly, yet another tweak has been made in the regulation, prescribing 10 acres as the new minimum campus size for 9 cities including the main metros. With this, the stage is set for corporate entities like Max Healthcare, the Apollo Group, and Fortis Healthcare to enter the medical education market.
The new regulations will not be a surprise to corporate bodies in the healthcare industry. Over two years back, the Health Ministry of the Government of India had gone public with its desire to relax land norms and allow corporate houses to open medical colleges.
Until now, medical education in India has been projected as a not-for-profit activity to be organised for the public good. While private bodies can run medical colleges, these can only be societies or trusts, legally non-profit organizations. (It is a different matter that illegal donations are collected.) In opening the door to corporate colleges, thus, a major policy change has been effected without changing the law or even a discussion in Parliament, but by simply getting a compliant MCI to change the regulation on establishment of medical colleges.
Colleges without faculty
This and other changes (such as recognising medical practitioners trained in five English-speaking countries including the US and UK) have been justified in the name of addressing the shortage of doctors. At the same time, over 50 existing medical colleges, including 15 run by the government, have been prohibited from admitting students in 2010 for having failed to meet the basic standards prescribed. Ninety per cent of these colleges have come up in the last 5 years.
Particularly shocking is the phenomenon of government colleges falling short of standards approved by the Government. Chattisgarh has three medical colleges, all run by the Government. Of these, two have been found unfit. In Madhya Pradesh, three of the six and in Karnataka four of the 10 government medical colleges have been found unfit. The list even includes a 50-year-old medical college in Jabalpur. The number of students admitted to the MBBS program has remained virtually stagnant - 28,349 in 2006 versus 28,742 in 2010 - though there are nominally 40 more colleges now compared to 2006!
Why are (state) government institutions not able to meet the requirements that have been approved by the (central) government? A severe problem faced by government-run institutions is attracting and retaining teaching faculty, and this is likely to be among the major reasons for these colleges failing to satisfy the MCI norms. The crisis building up on the faculty front has been flagged by various commissions looking into problems of medical education over the years, including the Knowledge Commission in 2006.
An indicator of the crisis is the attempt to conjure up faculty when MCI carries out inspections of new colleges, one of its regulatory functions. Judging by news reports, the practice of presenting fake faculty - students or private medical practitioners hired for the day - during MCI inspections in private colleges is common. What is interesting is that even government colleges are adopting unscrupulous methods. According to a news report (Times of India, April 29, 2010), the Karnataka Government could not find faculty for six newly opened medical colleges in Mandya, Hassan, Shimoga, Bellary, Bidar and Raichur after admitting students, reportedly because government pay scales were not competitive. Faculty were transferred temporarily from established medical colleges in cities like Bangalore and Hubli to the new colleges to be present during the MCI inspections with a commitment that they would be back to their original posts after the inspection was over.

The practice of presenting fake faculty - students or private medical practitioners hired for the day - during MCI inspections in private colleges is common.

The government's response to the shortage of faculty has been little short of a stroke of genius. Post-graduate seats in medical colleges have been increased dramatically by getting the MCI to change the 'standard' - the stipulated maximum ratio of students to teachers in postgraduate courses. Ironically, many state governments have been slow to respond to the MCI's liberal attitude; there may be other more basic constraints to be overcome before they can accept more students, it seems.
Unfavourable global comparisons
How does India compare with other countries, with respect to the numbers of doctors? The table below shows World Health Organization (WHO) figures for the density of doctors & specialists, and the density of trained nurses & midwives, as well as certain mother and child health indicators. India has the worst health indicators as well as the lowest numbers of doctors PLUS nurses for every 10,000 people. The density of doctors, at 6 per 10,000 (not including ayurvedic and homeopathic practitioners), is expectedly far below the numbers for developed countries. The density of nurses in comparison with the developed countries is even more glaring.
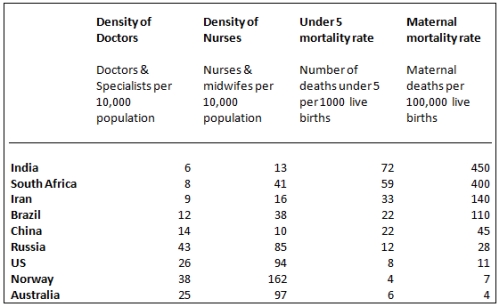
Density of health workers and certain health indicators in select countries.
(Data sourced from the WHO).
What about the comparison with Brazil, China, Russia, and South Africa, a favourite game among those enamored with GDP growth rates? The numbers speak for themselves. What will come as a surprise to many is that South Africa is marginally better than India in health indicators and has a better health worker density. While the health indicators depend on various factors including nutrition and hygiene, it is in some measure also linked to the availability of health workers.
Health centers without doctors and nurses
Even the poor picture above does not reveal the true situation in rural India. Only a fraction of the doctors and nursing professionals serve rural areas where 70 per cent of our population lives. Rural healthcare provided by the government has a three-tier structure - Sub Centre, Primary Heath Centre (PHC) and the Community Health Centre (CHC). The PHC is the first place available for the rural poor to see a doctor. Each PHC serves on average a population greater than 31,000 and must have at least one doctor and one nurse. For specialist consultation, people are expected to go to the CHC. Each CHC serves on average a population greater than 1.7 lakhs and must have 4 specialists â a surgeon, gynecologist, physician and pediatrician â supported by 7 nurses.
These heath care centers are grossly inadequate in number. By the Government's own admission, it needs to establish 50 per cent more CHCs. But even at the current abysmal level of service, a large number of positions of health workers remain unfilled in rural health centres - there are 3537 doctors' posts lying vacant, 11,033 similarly vacant for specialists, and 18,021 more vacancies for nurses and midwives (2008 data).
The Health Ministry, with the help of the MCI, has been active in proposing yet another 'innovative' solution to the problem of lack of doctors in the rural areas. The proposal is for a three-and-a-half year course to obtain the degree of Bachelor of Rural Medicine and Surgery (BRMS). Only rural candidates would be able to join this course. The study and training would happen at two different levels - Community Health Centers for 18 months, and sub-divisional hospitals for a further period of 2 years - and be conducted by retired professors. After completion of training, they would only be able to serve in their own state in district hospitals, community health centres, and primary health centres.
A cynical critic may well paraphrase the thinking behind this proposal this way. "Since we cannot invest more to upgrade rural hospitals and provide doctors and specialists with a competitive salary and a good work environment, we may as well dispense with them all together. We will instead train a new type of health worker in the existing rural health facilities and employ him in the same facilities. He will be more or less a bonded employee, as we will not permit him to practice outside the state or even move to urban hospitals within his state. Since we cannot pay enough to attract teaching faculty, we will use retired professors to train these rural medics; that and a shorter course will reduce the need for faculty and also bring down the cost."
The BRMS proposal has invited sharp criticism from some doctors' organizations on the grounds that it is discriminatory to have two different standards of health care - one for urban and the other for rural areas, and that the health care provided by such graduates will be compromised. At the other end is the opinion expressed by some that "something is better than nothing", that since doctors do not want to serve in rural areas, the government may as well create a new cadre of medics who will be obliged to serve there. The debate will surely pick up after the government formally lays out its plans. What is apparent is that neither this proposal nor the various stopgap measures adopted so far address the root of the problem of health care.
Corruption is certainly a major issue that affects the standards of medical education and the credibility of the regulator. However, the far larger issue is government policy, the low priority attached by the government to the social sector as a whole and the health sector in particular, evidenced in the paltry allocations for maintaining and upgrading medical infrastructure and medical education and for looking after precious human resources.